
Jul 16, 2026Technical Insights
Best Wavelength for Red Light Therapy? A Guide for Device Makers
Best wavelength for red light therapy devices: matching 630–680nm red to skin and scalp targets, and knowing when near-infrared is required.
1ONELASER develops visible-red VCSEL light-source solutions for device OEMs, from bare die and SMD packages through custom package and array design. For red light therapy and photobiomodulation (PBM) devices, 660nm is the most commonly selected red wavelength, and the 630–680nm band covers most skin, scalp, and other superficial applications. Targets below the dermis need near-infrared rather than more red. Choosing the best wavelength for red light therapy is an engineering input tied to the target tissue, not a bigger-is-better spec, and getting it wrong shows up as a validation or compliance problem rather than a matter of taste.
Wavelength is a design input, not a bigger-is-better number
First, a boundary: this is a sourcing question, not a shopping one. For a finished panel you buy off the shelf, total output and how you use it matter more than the exact nm. For a device you build, the wavelength is a hard input, and it comes from biology rather than preference.
Light can only drive a photochemical effect if something absorbs it. In PBM, the most widely discussed candidate for that absorber is cytochrome c oxidase (CCO), the terminal enzyme of the mitochondrial electron transport chain. It is worth stating plainly that this is a leading hypothesis and not a closed question. Reviews have proposed mechanisms beyond cytochrome c oxidase, including light and heat-gated ion channels, opsins, and structured water, and the evidence has been challenged by authors who note that no reliable demonstration of a light-induced mechanistic effect on CCO has been reported.
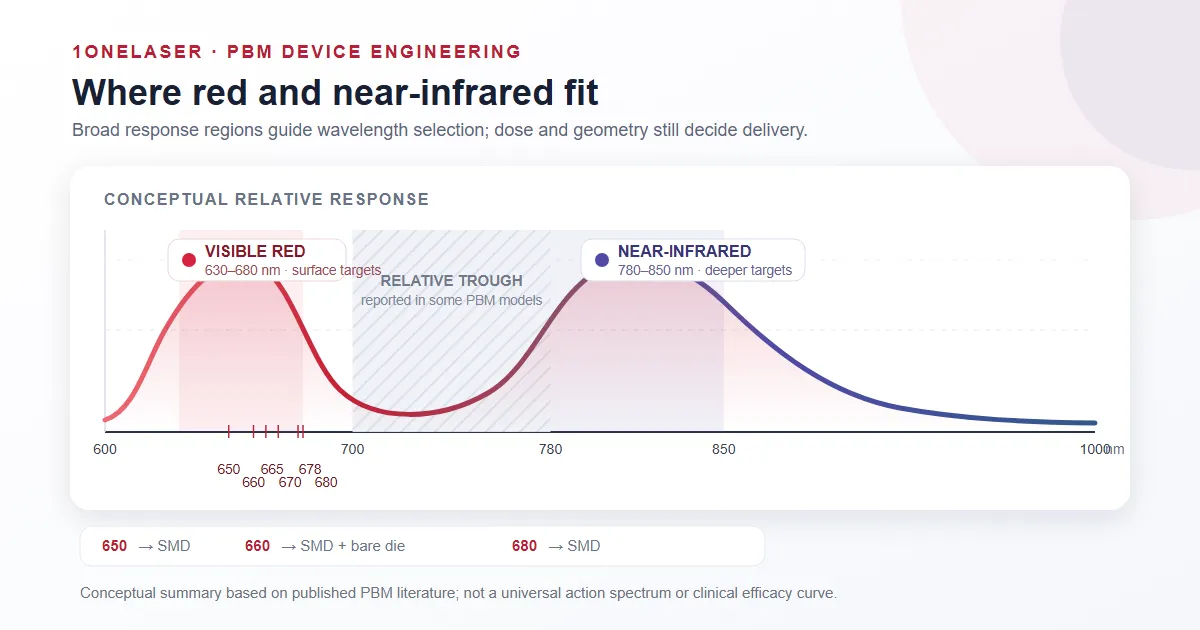
For a component decision that ambiguity is manageable, because it does not change the engineering. Whatever the receptor turns out to be, the reported absorption in the red and near-infrared is band-structured rather than flat: response regions cluster in the red around 620–680nm and in the near-infrared around 780–850nm, with a relative trough between them. Treat those as broad biological response windows rather than an exact universal curve, because reported values shift with tissue, dose, and experimental model. The design rule that survives all of it is the same: pick the wavelength from the target tissue, then design the dose.
The red band, wavelength by wavelength
Inside 630–680nm the reported biological differences are modest, but that does not make the wavelengths interchangeable. Each has a practical home, and each should be evaluated against the evidence for your specific application rather than swapped on the assumption that red is red.
- 630nm: the shallowest visible red. Surface skin and early collagen work; least penetration and the most competition from melanin absorption.
- 650nm: the visible-red and hair workhorse, and the reference point for cleared low-level laser therapy hair devices. It is also where surface-mount parts replace legacy TO-can red laser diodes.
- 660nm: the most commonly selected red wavelength for PBM product development. It sits on the reported red response region and is the most studied of the band.
- 665–670nm: close to 660nm in reported behavior, sometimes chosen for dermatology or marginally deeper red; available as bare die.
- 678–680nm: the top of the visible-red window, used in scalp and hair devices and where slightly more penetration or higher per-emitter output helps. 680nm is available at higher output.
Across the band, wavelength should be evaluated together with irradiance, dose, treatment geometry, and uniformity. A 10 to 20nm wavelength difference on its own does not determine finished-device performance. Pick the wavelength for the tissue, then stop optimizing nm and start optimizing dose.
Where red stops and near-infrared begins
Red light in the 630–680nm band is a surface-tissue tool. How far it actually gets is not a fixed number, and this is where most spec sheets and most marketing go wrong.
Published penetration figures for 660nm range from roughly 2mm to several centimeters. They are not contradicting each other. They are answering different questions. Light in tissue decays exponentially rather than stopping at a boundary, so any "depth" figure is really a statement about where someone chose to put the threshold, and it moves with skin pigmentation, blood content, spot size, incidence angle, irradiance, contact versus non-contact delivery, and whether the measurement was optical transmission or biological response.
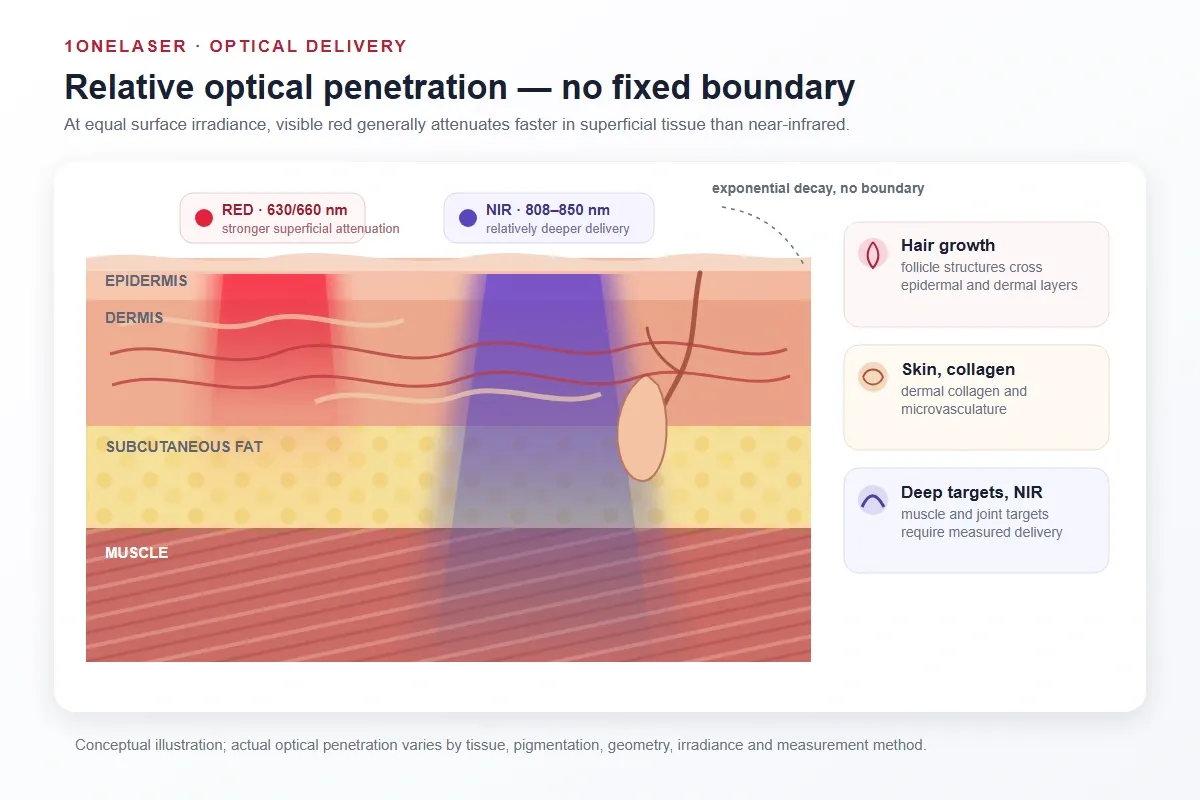
So the useful question for a device is not how deep the light goes. It is what irradiance survives to your target depth, in your geometry, on your patient population, which is measured rather than looked up.
What is consistent across methods is the ordering. At equal surface irradiance, visible red is absorbed and scattered more strongly in superficial tissue than the near-infrared wavelengths around 808–850nm, and melanin absorbs visible red more strongly than near-infrared, which adds variability across skin tones. For targets below the dermis, muscle, joints, and tendons, red is the wrong tool and the bill of materials needs an NIR emitter too. The 700–780nm range between the two commonly used regions falls in a reported relative trough and is less common in commercial and research systems, though that is a statement about where the evidence base sits rather than a claim that every wavelength in it is inactive.
Wavelength picks the door, dose and uniformity decide the result
Choosing 660nm only sets which part of the response region you are aiming at. Whether the tissue receives a useful dose depends on irradiance at the target (mW/cm²), exposure time (fluence, J/cm²), and how evenly the light covers the treatment area. PBM also follows a biphasic dose response, so past an optimum the reported effect falls away, which means more is not automatically better. Two emitter properties shape this.
First, wavelength precision and directionality. The red VCSEL parts in this series are specified at ±10nm, with ±5nm or ±2nm binning available on request, against ±20nm to ±30nm typical for a red LED. A laser also emits a narrow line, while an LED emits a band tens of nanometers wide, so more of a VCSEL’s output lands where you aimed it. Divergence for these parts runs 18° to 20°, against roughly 120° for a bare Lambertian LED, which puts energy on the treatment area instead of spilling sideways. Those figures describe the parts in this series and the applicable datasheet, not VCSELs and LEDs as categories: tolerance, spectral width, and divergence all depend on die, package, and optics on either side.
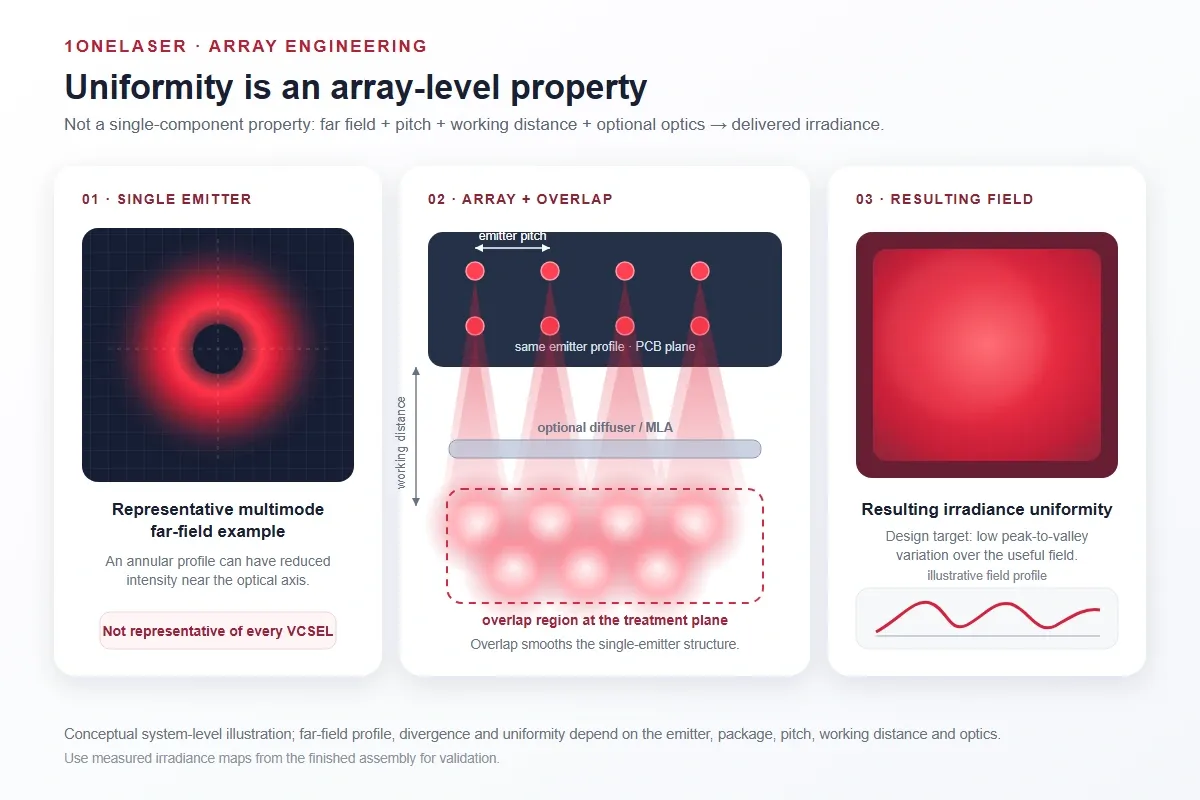
Second, beam shape. Multimode VCSEL designs, including the parts in this series, can produce an annular or doughnut-shaped far field with reduced intensity near the optical axis. Uniform illumination is therefore a system property rather than a single-emitter one: many emitters on a regular pitch whose spots overlap at the working distance, with a diffuser or micro-lens array when the pitch cannot come down. A precise wavelength only pays off if the array delivers it evenly, which is a package, power, and layout decision covered on its own.
Matching a wavelength to a manufacturable emitter
Once the wavelength is set, two questions decide whether it can be built as specified: does it exist in a format your line can place, and how tightly can it be held across a production run?
Check format availability before the wavelength is locked, not after. Teams that place finished parts need the wavelength in a surface-mount package. Teams that build their own package or module need it as bare die. The red band is not served identically in both formats at every wavelength, and finding that out late means either re-opening a wavelength decision you thought was closed, or taking on packaging work you did not plan for.
Across 630–680nm the availability maps out like this: 650nm as a 650nm VCSEL SMD series in several package sizes for hair-growth and visible-red boards; 660nm as both a 660nm VCSEL SMD series in 5mW and 7mW classes and a 660nm bare die in single and multi-emitter dies; and the upper band as a 680nm VCSEL SMD series for scalp and higher-output uses.
Then tolerance. A tight bin keeps every unit on the same part of the response region, so device output stays consistent unit to unit. Where a catalog part cannot meet the format, pitch, or tolerance a design needs, custom packaging becomes an engineering answer rather than a purchasing preference. That is the kind of project 1ONELASER typically supports.
One boundary is worth stating plainly. The emitter is a component. The finished-device manufacturer remains responsible for optical-dose validation, laser-safety classification, applicable photobiological risk assessment, product testing, labeling, and any clinical or marketing claims. Standards such as IEC 60825-1 may be relevant to laser product classification depending on the finished product and jurisdiction. A supplier provides the light source and its specifications, not therapeutic performance.
FAQ
What is the best wavelength for red light therapy?
660nm is the most commonly selected red wavelength for skin and surface PBM, and the 630–680nm band covers most skin, scalp, and other superficial applications. Targets below the dermis need near-infrared around 808–850nm rather than a longer red wavelength. Wavelength should be chosen from the target tissue and then evaluated together with irradiance, dose, and uniformity.
Is 660nm better than 630nm?
Reported effects across 630–670nm are broadly similar, and 660nm is the most studied of the band, but that does not make them interchangeable for a given application. Both should be assessed against the evidence for your indication. In practice, delivered dose and uniformity separate finished devices far more than a 30nm wavelength difference.
How deep does 660nm red light penetrate?
There is no single number. Published figures for 660nm range from roughly 2mm to several centimeters, because light decays exponentially in tissue and any depth figure depends on the threshold chosen and on pigmentation, geometry, irradiance, and measurement method. The consistent finding is the ordering: visible red is absorbed more superficially than near-infrared. For a device, measure the irradiance that survives to your target depth rather than looking up a depth.
What wavelength do hair-growth devices use?
A systematic review of FDA-cleared home-use devices identified 32 such low-level light therapy devices as of January 2020, and cleared devices have clustered on red laser diodes at roughly 635, 650, and 655nm, with at least one at 678nm. That makes the low-650s an established reference point for low-level laser hair-growth systems.
Why is 700–780nm less common in PBM devices?
Reported response regions cluster in the red around 620–680nm and in the near-infrared around 780–850nm, with a relative trough between them, which is one reason commercial and research systems more commonly select wavelengths in those two regions. It is not a universal statement that every wavelength in 700–780nm is biologically inactive.
Do you need near-infrared as well as red?
For surface targets, no. For muscle, joints, and deeper tissue, visible red is absorbed too superficially to be the right tool, and many devices pair a red wavelength with an NIR wavelength around 808–850nm.
Can different wavelengths be combined in one module?
Yes, and for red plus near-infrared designs it is often the practical route. The alternative is two emitter populations, two pitches, and two thermal footprints on one board. A multi-wavelength VCSEL SMD carries red and near-infrared in a single package with independently driven channels, which keeps one placement population and lets firmware sequence the bands instead of the layout fixing the ratio. The trade is that you take the ratio the package gives you, where discrete emitters let you tune the count of each band independently.
Does 1ONELASER support red VCSEL designs at these wavelengths?
Yes. The visible-red band from 650 to 680nm is available as bare die and surface-mount packages for OEM integration, with custom package, array, and binning options where a catalog part does not fit the design. The device maker validates the finished product and owns any clinical or regulatory claims.
Pick the wavelength from the tissue, hold a tight bin across the production run, and design the array for even dose. For emitter selection, 1ONELASER develops red VCSEL light sources from 650 to 680nm in bare die, SMD, and custom package or array form, with evaluation kits available for design-in testing.